
Topic 1.6. Overview of quality of life in Friedreich ataxia
This chapter of the Clinical Management Guidelines for Friedreich Ataxia and the recommendations and best practice statements contained herein were endorsed by the authors and the Friedreich Ataxia Guidelines Panel in 2022.
Topic Contents
1.6 Overview of quality of life in Friedreich ataxia
1.6.1 Background
1.6.2 Literature review
Disclaimer / Intended Use / Funding
Disclaimer
The Clinical Management Guidelines for Friedreich ataxia (‘Guidelines’) are protected by copyright owned by the authors who contributed to their development or said authors’ assignees.
These Guidelines are systematically developed evidence statements incorporating data from a comprehensive literature review of the most recent studies available (up to the Guidelines submission date) and reviewed according to the Grading of Recommendations, Assessment Development and Evaluations (GRADE) framework © The Grade Working Group.
Guidelines users must seek out the most recent information that might supersede the diagnostic and treatment recommendations contained within these Guidelines and consider local variations in clinical settings, funding and resources that may impact on the implementation of the recommendations set out in these Guidelines.
The authors of these Guidelines disclaim all liability for the accuracy or completeness of the Guidelines, and disclaim all warranties, express or implied to their incorrect use.
Intended Use
These Guidelines are made available as general information only and do not constitute medical advice. These Guidelines are intended to assist qualified healthcare professionals make informed treatment decisions about the care of individuals with Friedreich ataxia. They are not intended as a sole source of guidance in managing issues related to Friedreich ataxia. Rather, they are designed to assist clinicians by providing an evidence-based framework for decision-making.
These Guidelines are not intended to replace clinical judgment and other approaches to diagnosing and managing problems associated with Friedreich ataxia which may be appropriate in specific circumstances. Ultimately, healthcare professionals must make their own treatment decisions on a case-by-case basis, after consultation with their patients, using their clinical judgment, knowledge and expertise.
Guidelines users must not edit or modify the Guidelines in any way – including removing any branding, acknowledgement, authorship or copyright notice.
Funding
The authors of this document gratefully acknowledge the support of the Friedreich Ataxia Research Alliance (FARA). The views and opinions expressed in the Guidelines are solely those of the authors and do not necessarily reflect the official policy or position of FARA.
1.6 Overview of quality of life in Friedreich ataxia
Jennifer Farmer, Elisabetta Soragni and Myriam Rai
1.6.1 Background
Quality of life (QOL) in FRDA is influenced by many different factors, not the least of which is living with a chronic, progressive disease. Being able to quantify health-related QOL issues is essential to clinical research and long-term evaluation of the impact of new treatments and guideline recommendations. This section covers specific issues related to QOL in individuals with FRDA; in particular, techniques and equipment that promote health and independence in a person with FRDA, and the presence and management of mental health and psychological symptoms related to FRDA. Specific attention is given to medical management in the later stages of the disease process when QOL is the driving focus of medical decision making.
1.6.2 Literature review
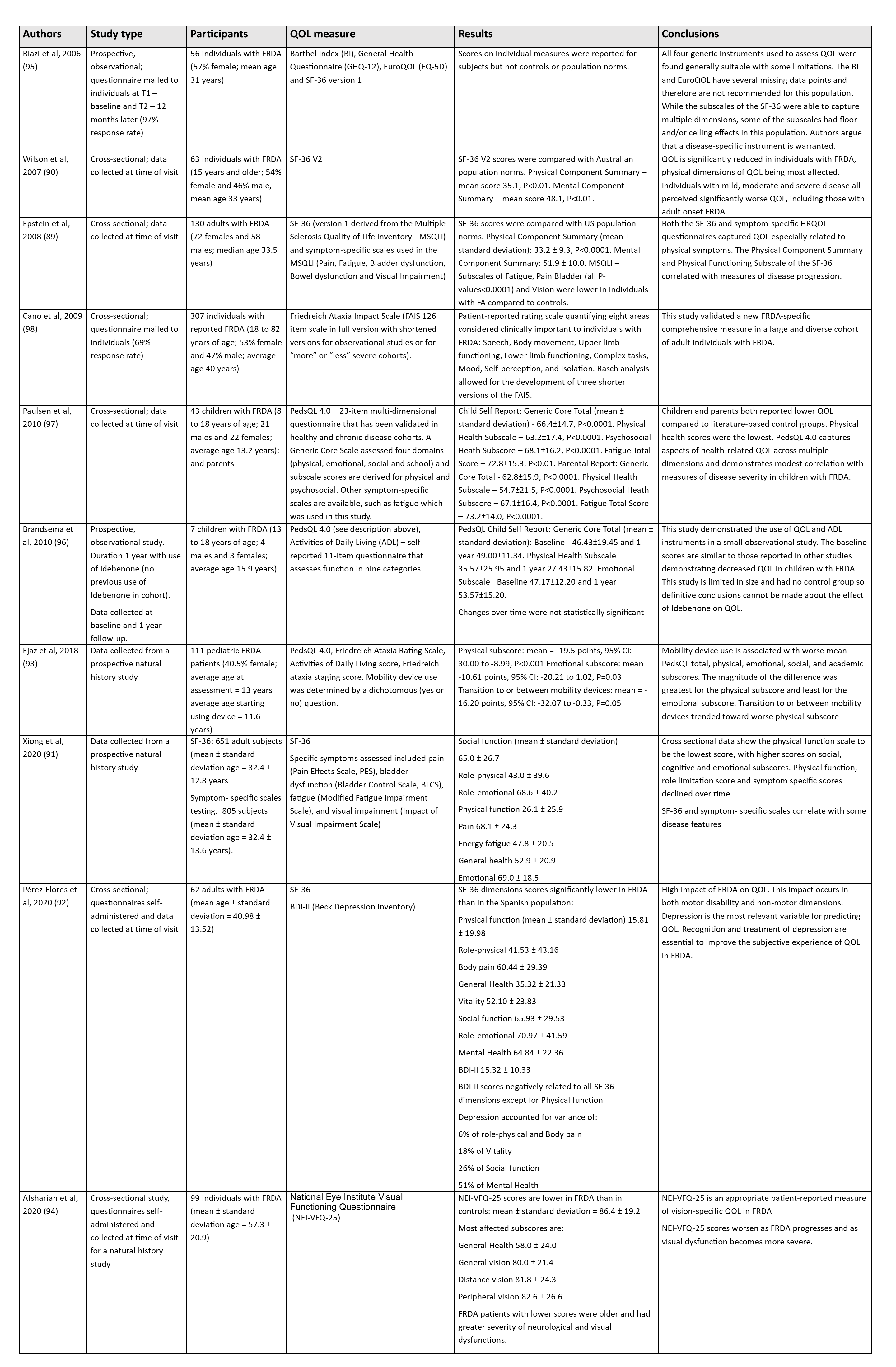
There are only a handful of studies specifically evaluating QOL in individuals with FRDA. Findings from these studies are summarized in Table 1.4.
There is no doubt that FRDA is associated with decreased QOL. The Australian and US studies have very similar findings, utilizing the SF-36 to quantify QOL in diverse cross-sectional cohorts of adults with FRDA (89, 90). The SF-36, while not specific to FRDA, is able to capture QOL at various stages of disease (89, 90). While physical components have worse scores, both physical and mental components of health-related QOL are decreased in individuals with FRDA in various stages of disease (89, 90). Even those with milder stage and/or late onset FRDA reported decreased QOL (90). A more recent large study in a heterogeneous cohort confirmed these observations and showed a correlation between physical scales and some disease features and their decline over time (91). When depression symptoms are analyzed, these scores are predictive of QOL (92). A study analyzing the association between mobility device use in children with FRDA and their health-related QOL shows that mobility device use is associated with worse QOL outcomes, with the effect being greatest for physical functioning (93). Worsening of academic, social, and emotional functioning also suggests that use of mobility devices has important psychosocial implications for children with FRDA. A more recent study (94) has determined an association of patient-reported vision-specific QOL with visual function and disease status in FRDA. The 25-Item National Eye Institute Visual Functioning Questionnaire (NEI-VFQ-25) was significantly lower (indicating worse QOL) in FRDA compared to other controls groups. Rank correlations revealed lower NEI-VFQ-25 scores among patients with greater disease severity (94).
The results from these studies should signal to a clinician that from the point of diagnosis onward individuals with FRDA may have decreased QOL, which may impact on other aspects of life including psychological function. Any adjunctive support that can improve an individual’s symptoms, especially physical symptoms such as reduced ambulation, fatigue or pain, could improve QOL.
For more information, see Chapter 16: Digital and assistive technologies in Friedreich ataxia.
In reviewing QOL studies, it is important to note the range of instruments used to measure QOL in FRDA. The SF-36 (in various versions) has been used most often for adult participants (89, 90, 95). In pediatric cohorts, the PedsQL has been used to assess QOL (96, 97). This instrument offers both child report questionnaires based on age and parental report questionnaire. In addition, there has been research to develop a disease-specific instrument, the Friedreich’s Ataxia Impact Scale or FAIS (98), but it has not yet been used widely.
Table 1.4 Literature review of general quality of life in Friedreich ataxia
Jennifer Farmer, MS
Chief Executive Officer, Friedreich’s Ataxia Research Alliance (FARA), Downingtown, Pennsylvania, USA
Email: info@curefa.org
Myriam Rai, PhD
Director of Global Relations & Initiatives, Friedreich’s Ataxia Research Alliance (FARA), Brussels, Belgium
Email: myriam.rai@curefa.org
Elisabetta Soragni
Director of Research, The Friedreich’s Ataxia Research Alliance, Downingtown, Pennsylvania, USA
Email: liz.soragni@curefa.org
2. Friedreich N. Uber degenerative Atrophie der spinalen Hinterstrange. Virchow’s Arch Path Anat. 1863;26:291-419.
3. Friedreich N. Uber degenerative Atrophie der spinalen Hinterstrange. Virchow’s Arch Path Anat. 1863;27:1-26.
4. Friedreich N. Uber degenerative Atrophie der spinalen Hinterstrange. Virchow’s Arch Path Anat. 1863;26:433-59.
5. Friedreich N. Uber ataxie mit besonderer berucksichtigung der herditaren formen. Virchow’s Arch Path Anat. 1876;68:145-245.
6. Friedreich N. Uber ataxie mit besonderer berucksichtigung der hereditaren formen. Virchow’s Arch Path Anat. 1877;70:140-52.
7. Campuzano V, Montermini L, Molto MD, Pianese L, Cossee M, Cavalcanti F, et al. Friedreich’s ataxia: autosomal recessive disease caused by an intronic GAA triplet repeat expansion. Science. 1996;271(5254):1423-7.
8. Reetz K, Dogan I, Costa AS, Dafotakis M, Fedosov K, Giunti P, et al. Biological and clinical characteristics of the European Friedreich’s Ataxia Consortium for Translational Studies (EFACTS) cohort: a cross-sectional analysis of baseline data. Lancet Neurol. 2015;14(2):174-82.
9. Geoffroy G, Barbeau A, Breton G, Lemieux B, Aube M, Leger C, et al. Clinical description and roentgenologic evaluation of patients with Friedreich’s ataxia. Can J Neurol Sci. 1976;3(4):279-86.
10. Harding AE. Friedreich’s ataxia: a clinical and genetic study of 90 families with an analysis of early diagnostic criteria and intrafamilial clustering of clinical features. Brain. 1981;104(3):589-620.
11. Dürr A, Cossee M, Agid Y, Campuzano V, Mignard C, Penet C, et al. Clinical and genetic abnormalities in patients with Friedreich’s ataxia. N Engl J Med. 1996;335(16):1169-75.
12. Schöls L, Amoiridis G, Przuntek H, Frank G, Epplen JT, Epplen C. Friedreich’s ataxia. Revision of the phenotype according to molecular genetics. Brain. 1997;120(Pt 12):2131-40.
13. Bürk K. Friedreich ataxia: current status and future prospects. Cerebellum Ataxias. 2017;4:4.
14. Rummey C, Farmer JM, Lynch DR. Predictors of loss of ambulation in Friedreich’s ataxia. EClinicalMedicine. 2020;18:100213.
15. Delatycki MB, Paris DB, Gardner RJ, Nicholson GA, Nassif N, Storey E, et al. Clinical and genetic study of Friedreich ataxia in an Australian population. Am J Med Genet. 1999;87(2):168-74.
16. Rosen KM, Folker JE, Vogel AP, Corben LA, Murdoch BE, Delatycki MB. Longitudinal change in dysarthria associated with Friedreich ataxia: a potential clinical endpoint. J Neurol. 2012;259(11):2471-7.
17. Ribaï P, Pousset F, Tanguy M, Rivaud-Pechoux S, Le Ber I, Gasparini F, et al. Neurological, cardiological, and oculomotor progression in 104 patients with Friedreich ataxia during long-term follow-up. Arch Neurol. 2007;64:558-64.
18. Patel M, Isaacs CJ, Seyer L, Brigatti K, Gelbard S, Strawser C, et al. Progression of Friedreich ataxia: quantitative characterization over 5 years. Ann Clin Transl Neurol. 2016;3(9):684-94.
19. Delatycki MB, Corben LA. Clinical features of Friedreich ataxia. J Child Neurol. 2012;27(9):1133-7.
20. Musegante A, Almeda P, Monteiro R, Bassoro U. Urinary symptoms and urodynamics findings in patients with Friedreich’s ataxia. International Brazilian Journal of Urology. 2013;39(6):867-74.
21. McCabe DJ, Ryan F, Moore DP, McQuaid S, King MD, Kelly A, et al. Typical Friedreich’s ataxia without GAA expansions and GAA expansion without typical Friedreich’s ataxia.[erratum appears in J Neurol 2000 Jun;247(6):483]. J Neurol. 2000;247(5):346-55.
22. Tsou AY, Paulsen EK, Lagedrost SJ, Perlman SL, Mathews KD, Wilmot GR, et al. Mortality in Friedreich ataxia. J Neurol Sci. 2011;307:46-9.
23. Pousset F, Legrand L, Monin ML, Ewenczyk C, Charles P, Komajda M, et al. A 22-year follow-up study of long-term cardiac outcome and predictors of survival in Friedreich ataxia. JAMA Neurol. 2015;72(11):1334-41.
24. Fortuna F, Barboni P, Liguori R, Valentino ML, Savini G, Gellera C, et al. Visual system involvement in patients with Friedreich’s ataxia. Brain. 2009;132(Pt 1):116-23.
25. Rance G, Fava R, Baldock H, Chong A, Barker E, Corben L, et al. Speech perception ability in individuals with Friedreich ataxia. Brain. 2008;131:2002-12.
26. Galea CA, Huq A, Lockhart PJ, Tai G, Corben LA, Yiu EM, et al. Compound heterozygous FXN mutations and clinical outcome in Friedreich ataxia. Ann Neurol. 2016;79(3):485-95.
27. Colombo R, Carobene A. Age of the intronic GAA triplet repeat expansion mutation in Friedreich ataxia. Hum Genet. 2000;106(4):455-8.
28. Campuzano V, Montermini L, Lutz Y, Cova L, Hindelang C, Jiralerspong S, et al. Frataxin is reduced in Friedreich ataxia patients and is associated with mitochondrial membranes. Hum Mol Genet. 1997;6(11):1771-80.
29. Li Y, Lu Y, Polak U, Lin K, Shen J, Farmer J, et al. Expanded GAA repeats impede transcription elongation through the FXN gene and induce transcriptional silencing that is restricted to the FXN locus. Hum Mol Genet. 2015;24(24):6932-43.
30. Rodden LN, Chutake YK, Gilliam K, Lam C, Soragni E, Hauser L, et al. Methylated and unmethylated epialleles support variegated epigenetic silencing in Friedreich ataxia. Hum Mol Genet. 2021;29(23):3818-29.
31. Herman D, Jenssen K, Burnett R, Soragni E, Perlman SL, Gottesfeld JG. Histone deacetylase inhibitors reverse gene silencing in Friedreich’s ataxia. Nat Chem Biol. 2006;2(10):551-8.
32. Li L, Matsui M, Corey DR. Activating frataxin expression by repeat-targeted nucleic acids. Nat Commun. 2016;7:10606.
33. Gervason S, Larkem D, Mansour AB, Botzanowski T, Muller CS, Pecqueur L, et al. Physiologically relevant reconstitution of iron-sulfur cluster biosynthesis uncovers persulfide-processing functions of ferredoxin-2 and frataxin. Nat Commun. 2019;10(1):3566.
34. Gonzalez-Cabo P, Palau F. Mitochondrial pathophysiology in Friedreich’s ataxia. J Neurochem. 2013;126 Suppl 1:53-64.
35. Koeppen AH. Friedreich’s ataxia: pathology, pathogenesis, and molecular genetics. J Neurol Sci. 2011;303(1-2):1-12.
36. Harding IH, Lynch DR, Koeppen AH, Pandolfo M. Central nervous system therapeutic targets in Friedreich ataxia. Hum Gene Ther. 2020;31(23-24):1226-36.
37. Koeppen AH, Becker AB, Qian J, Feustel PJ. Friedreich Ataxia: Hypoplasia of Spinal Cord and Dorsal Root Ganglia. J Neuropathol Exp Neurol. 2017;76(2):101-8.
38. Koeppen AH, Becker AB, Qian J, Gelman BB, Mazurkiewicz JE. Friedreich Ataxia: Developmental Failure of the Dorsal Root Entry Zone. J Neuropathol Exp Neurol. 2017;76(11):969-77.
39. Dogan I, Romanzetti S, Didszun C, Mirzazade S, Timmann D, Saft C, et al. Structural characteristics of the central nervous system in Friedreich ataxia: an in vivo spinal cord and brain MRI study. J Neurol Neurosurg Psychiatry. 2019;90(5):615-7.
40. Dogan I, Tinnemann E, Romanzetti S, Mirzazade S, Costa AS, Werner CJ, et al. Cognition in Friedreich’s ataxia: a behavioral and multimodal imaging study. Ann Clin Transl Neurol. 2016;3(8):572-87.
41. Lindig T, Bender B, Kumar VJ, Hauser TK, Grodd W, Brendel B, et al. Pattern of cerebellar atrophy in Friedreich’s ataxia-using the SUIT template. Cerebellum. 2019;18(3):435-47.
42. Rezende TJR, Martinez ARM, Faber I, Girotto Takazaki KA, Martins MP, de Lima FD, et al. Developmental and neurodegenerative damage in Friedreich’s ataxia. Eur J Neurol. 2019;26(3):483-9.
43. Selvadurai LP, Corben LA, Delatycki MB, Storey E, Egan GF, Georgiou-Karistianis N, et al. Multiple mechanisms underpin cerebral and cerebellar white matter deficits in Friedreich ataxia: The IMAGE-FRDA study. Hum Brain Mapp. 2020;41(7):1920-33.
44. Vavla M, Arrigoni F, Nordio A, De Luca A, Pizzighello S, Petacchi E, et al. Functional and structural brain damage in Friedreich’s ataxia. Front Neurol. 2018;9:747.
45. Ward PGD, Harding IH, Close TG, Corben LA, Delatycki MB, Storey E, et al. Longitudinal evaluation of iron concentration and atrophy in the dentate nuclei in friedreich ataxia. Mov Disord. 2019;34(3):335-43.
46. Gramegna LL, Tonon C, Manners DN, Pini A, Rinaldi R, Zanigni S, et al. Combined cerebellar proton MR spectroscopy and DWI study of patients with Friedreich’s ataxia. Cerebellum. 2017;16(1):82-8.
47. Öz G, Harding IH, Krahe J, Reetz K. MR imaging and spectroscopy in degenerative ataxias: toward multimodal, multisite, multistage monitoring of neurodegeneration. Curr Opin Neurol. 2020;33(4):451-61.
48. Cocozza S, Costabile T, Tedeschi E, Abate F, Russo C, Liguori A, et al. Cognitive and functional connectivity alterations in Friedreich’s ataxia. Ann Clin Transl Neurol. 2018;5(6):677-86.
49. Survey of the delay in diagnosis for 8 rare diseases in Europe (‘EurordisCare2’) 2007 [Available from: https://www.eurordis.org/publication/survey-delay-diagnosis-8-rare-diseases-europe-‘eurordiscare2’.
50. Global Commission to End the Diagnostic Odyssey for Children with a Rare Disease. Ending the diagnostic odyssey for children with a rare disease: Global Commission year one report 2019 [Available from: https://www.globalrarediseasecommission.com/Report/.
51. Indelicato E, Nachbauer W, Eigentler A, Amprosi M, Matteucci Gothe R, Giunti P, et al. Onset features and time to diagnosis in Friedreich’s Ataxia. Orphanet J Rare Dis. 2020;15(1):198.
52. Filla A, De Michele G, Coppola G, Federico A, Vita G, Toscano A, et al. Accuracy of clinical diagnostic criteria for Friedreich’s ataxia. Mov Disord. 2000;15(6):1255-8.
53. Filla A, De Michele G, Cavalcanti F, Pianese L, Monticelli A, Campanella G, et al. The relationship between trinucleotide (GAA) repeat length and clinical features in Friedreich ataxia. Am J Hum Genet. 1996;59(3):554-60.
54. Filla A, DeMichele G, Caruso G, Marconi R, Campanella G. Genetic data and natural history of Friedreich’s disease: a study of 80 Italian patients. J Neurol. 1990;237(6):345-51.
55. De Michele G, Di Maio L, Filla A, Majello M, Cocozza S, Cavalcanti F, et al. Childhood onset of Friedreich ataxia: a clinical and genetic study of 36 cases. Neuropediatrics. 1996;27(1):3-7.
56. Hanna MG, Davis MB, Sweeney MG, Noursadeghi M, Ellis CJ, Elliot P, et al. Generalized chorea in two patients harboring the Friedreich’s ataxia gene trinucleotide repeat expansion. Mov Disord. 1998;13(2):339-40.
57. Spacey SD, Szczygielski BI, Young SP, Hukin J, Selby K, Snutch TP. Malaysian siblings with friedreich ataxia and chorea: a novel deletion in the frataxin gene. Can J Neurol Sci. 2004;31(3):383-6.
58. Zhu D, Burke C, Leslie A, Nicholson GA. Friedreich’s ataxia with chorea and myoclonus caused by a compound heterozygosity for a novel deletion and the trinucleotide GAA expansion. Mov Disord. 2002;17(3):585-9.
59. Rummey C, Corben LA, Delatycki MB, Subramony SH, Bushara K, Gomez CM, et al. Psychometric properties of the Friedreich Ataxia Rating Scale. Neurology Genetics. 2019;5(6):371.
60. Furman JM, Perlman S, Baloh RW. Eye movements in Friedreich’s ataxia. Arch Neurol. 1983;40(6):343-6.
61. Kirkham TH, Guitton D, Katsarkas A, Kline LB, Andermann E. Oculomotor abnormalities in Friedreich’s ataxia. Can J Neurol Sci. 1979;6(2):167-72.
62. Ell J, Prasher D, Rudge P. Neuro-otological abnormalities in Friedreich’s ataxia. J Neurol Neurosurg Psychiatry. 1984;47(1):26-32.
63. Lamont PJ, Davis MB, Wood NW. Identification and sizing of the GAA trinucleotide repeat expansion of Friedreich’s ataxia in 56 patients. Clinical and genetic correlates. Brain. 1997;120(Pt 4):673-80.
64. Konieczny MR, Senyurt H, Krauspe R. Epidemiology of adolescent idiopathic scoliosis. J Child Orthop. 2013;7(1):3-9.
65. Allam AM, Schwabe AL. Neuromuscular scoliosis. PM R. 2013;5(11):957-63.
66. Mary P, Servais L, Vialle R. Neuromuscular diseases: Diagnosis and management. Orthop Traumatol Surg Res. 2018;104(1S):S89-S95.
67. Ahluwalia M, Ho CY. Cardiovascular genetics: the role of genetic testing in diagnosis and management of patients with hypertrophic cardiomyopathy. Heart. 2021;107(3):183-9.
68. Stafford F, Thomson K, Butters A, Ingles J. Hypertrophic cardiomyopathy: Genetic testing and risk stratification. Curr Cardiol Rep. 2021;23(2):9.
69. Berciano J, Mateo I, De Pablos C, Polo JM, Combarros O. Friedreich ataxia with minimal GAA expansion presenting as adult-onset spastic ataxia. J Neurol Sci. 2002;194(1):75-82.
70. Bhidayasiri R, Perlman SL, Pulst SM, Geschwind DH. Late-onset Friedreich ataxia: phenotypic analysis, magnetic resonance imaging findings, and review of the literature. Arch Neurol. 2005;62(12):1865-9.
71. Fearon C, Lonergan R, Ferguson D, Byrne S, Bradley D, Langan Y, et al. Very-late-onset Friedreich’s ataxia: diagnosis in a kindred with late-onset cerebellar ataxia. Pract Neurol. 2020;20(1):55-8.
72. Lhatoo SD, Rao DG, Kane NM, Ormerod IE. Very late onset Friedreich’s presenting as spastic tetraparesis without ataxia or neuropathy. Neurology. 2001;56(12):1776-7.
73. Lecocq C, Charles P, Azulay JP, Meissner W, Rai M, N’Guyen K, et al. Delayed-onset Friedreich’s ataxia revisited. Mov Disord. 2016;31(1):62-9.
74. Schulz JB, Boesch S, Burk K, Durr A, Giunti P, Mariotti C, et al. Diagnosis and treatment of Friedreich ataxia: a European perspective. Nat Rev Neurol. 2009;5(4):222-34.
75. Selvadurai LP, Harding IH, Corben LA, Georgiou-Karistianis N. Cerebral abnormalities in Friedreich ataxia: A review. Neurosci Biobehav Rev. 2018;84:394-406.
76. Caruso G, Santoro L, Perretti A, Serlenga L, Crisci C, Ragno M, et al. Friedreich’s ataxia: electrophysiological and histological findings. Acta Neurol Scand. 1983;67(1):26-40.
77. Michel C, Collins C. Pediatric neuromuscular disorders. Pediatr Clin North Am. 2020;67(1):45-57.
78. Spittle AJ, FitzGerald T, Mentiplay B, Williams J, Licari M. Motor impairments in children: More than just the clumsy child. J Paediatr Child Health. 2018;54(10):1131-5.
79. Mateo I, Llorca J, Volpini V, Corral J, Berciano J, Combarros O. Expanded GAA repeats and clinical variation in Friedreich’s ataxia. Acta Neurol Scand. 2004;109(1):75-8.
80. Al-Mahdawi S, Ging H, Bayot A, Cavalcanti F, La Cognata V, Cavallaro S, et al. Large Interruptions of GAA Repeat Expansion Mutations in Friedreich Ataxia Are Very Rare. Front Cell Neurosci. 2018;12:443.
81. Berciano J, Mateo I, De Pablos C, Polo JM, Combarros O. Friedreich ataxia with minimal GAA expansion presenting as adult-onset spastic ataxia. J Neurol Sci. 2002;194(1):75-82.
82. Napierala M, Dere R, Vetcher A, Wells RD. Structure-dependent recombination hot spot activity of GAA.TTC sequences from intron 1 of the Friedreich’s ataxia gene. J Biol Chem. 2004;279(8):6444-54.
83. Bit-Avragim N, Perrot A, Schols L, Hardt C, Kreuz FR, Zuhlke C, et al. The GAA repeat expansion in intron 1 of the frataxin gene is related to the severity of cardiac manifestation in patients with Friedreich’s ataxia. J Mol Med. 2001;78(11):626-32.
84. Isnard R, Kalotka H, Durr A, Cossee M, Schmitt M, Pousset F, et al. Correlation between left ventricular hypertrophy and GAA trinucleotide repeat length in Friedreich’s ataxia. Circulation. 1997;95(9):2247-9.
85. Marty B, Naeije G, Bourguignon M, Wens V, Jousmaki V, Lynch DR, et al. Evidence for genetically determined degeneration of proprioceptive tracts in Friedreich ataxia. Neurology. 2019;93(2):e116-e24.
86. Monrós E, Molto MD, Martinez F, Canizares J, Blanca J, Vilchez JJ, et al. Phenotype correlation and intergenerational dynamics of the Friedreich ataxia GAA trinucleotide repeat. Am J Hum Genet. 1997;61(1):101-10.
87. Greeley NR, Regner S, Willi S, Lynch DR. Cross-sectional analysis of glucose metabolism in Friedreich ataxia. J Neurol Sci. 2014;342(1-2):29-35.
88. Cossée M, Dürr A, Schmitt M, Dahl N, Trouillas P, Allinson P, et al. Friedreich’s ataxia: point mutations and clinical presentation of compound heterozygotes. Ann Neurol. 1999;45(2):200-6.
89. Epstein E, Farmer JM, Tsou A, Perlman S, Subramony SH, Gomez CM, et al. Health related quality of life measures in Friedreich Ataxia. J Neurol Sci. 2008;272(1-2):123-8.
90. Wilson C, Fahey MC, Corben L A, Collins V, Churchyard A, Lamont PJ, et al. Quality of life in Friedreich Ataxia: what clinical, social and demographic factors are important? Eur J Neurol. 2007;14(9):1040-7.
91. Xiong E, Lynch AE, Corben LA, Delatycki MB, Subramony SH, Bushara K, et al. Health related quality of life in Friedreich Ataxia in a large heterogeneous cohort. J Neurol Sci. 2020;410:116642.
92. Perez-Flores J, Hernandez-Torres A, Monton F, Nieto A. Health-related quality of life and depressive symptoms in Friedreich ataxia. Qual Life Res. 2020;29(2):413-20.
93. Ejaz R, Chen S, Isaacs CJ, Carnevale A, Wilson J, George K, et al. Impact of mobility device use on quality of life in children with Friedreich ataxia. J Child Neurol. 2018;33(6):397-404.
94. Afsharian P, Nolan-Kenney R, Lynch AE, Balcer LJ, Lynch DR. Correlation of visual quality of life with clinical and visual status in Friedreich ataxia. J Neuroophthalmol. 2020;40(2):213-7.
95. Riazi A, Cano SJ, Cooper JM, Bradley JL, Schapira AH, Hobart JC. Coordinating outcomes measurement in ataxia research: do some widely used generic rating scales tick the boxes? Mov Disord. 2006;21(9):1396-403.
96. Brandsema JF, Stephens D, Hartley J, Yoon G. Intermediate-dose idebenone and quality of life in Friedreich ataxia. Pediatr Neurol. 2010;42(5):338-42.
97. Paulsen EK, Friedman LS, Myers LM, Lynch DR. Health-related quality of life in children with Friedreich ataxia. Pediatr Neurol. 2010;42(5):335-7.
98. Cano SJ, Riazi A, Schapira AH, Cooper JM, Hobart J. Friedreich’s ataxia impact scale: a new measure striving to provide the flexibility required by today’s studies. Mov Disord. 2009;24(7):984-2.
These Guidelines are systematically developed evidence statements incorporating data from a comprehensive literature review of the most recent studies available (up to the Guidelines submission date) and reviewed according to the Grading of Recommendations, Assessment Development and Evaluations (GRADE) framework © The Grade Working Group.
This chapter of the Clinical Management Guidelines for Friedreich Ataxia and the recommendations and best practice statements contained herein were endorsed by the authors and the Friedreich Ataxia Guidelines Panel in 2022.
It is our expectation that going forward individual topics can be updated in real-time in response to new evidence versus a re-evaluation and update of all topics simultaneously.